Documentation Bias in Clinical AI
Inconsistent clinical narratives, misclassification risk, and the data strategy needed to fix it.
1. Background
Clinical documentation has always carried more than diagnostic information. Embedded in every progress note, nursing flowsheet, and discharge summary is a layer of subjective clinical narrative shaped by the author’s tone, vocabulary, training, and unconscious assumptions about the patient in front of them. As healthcare systems increasingly rely on artificial intelligence to extract, summarize, and act on this narrative content, the inconsistency of that documentation has become a structural vulnerability rather than a stylistic quirk.
Documentation Bias refers to the systematic, often unintentional variation in how clinicians record patient encounters, symptoms, and behavior across different patient populations. The same clinical presentation can be described in markedly different language depending on the patient’s race, perceived socioeconomic status, insurance type, or behavioral history. This is not a hypothetical concern. A widely cited 2022 study of inpatient progress notes found that notes about non-Hispanic Black patients had a measurably greater probability of containing stigmatizing language than notes about non-Hispanic White patients with comparable diagnoses, even after adjusting for illness severity (Sun et al., 2022). A 2024 scoping review of the broader literature confirmed this is a consistent, replicated finding across multiple health systems and clinical settings, not an isolated result (Pérez et al., 2024).
Large language models trained on or deployed against this documentation inherit any inconsistencies, omissions, and tonal biases from the underlying notes. Generative AI scribes, clinical summarization tools, and natural language processing pipelines used for risk scoring or population health stratification do not distinguish between objective clinical facts and subjective framing unless they are explicitly designed to do so. The result is that Documentation Bias, originally a human authorship problem, becomes an algorithmic propagation problem the moment AI is introduced into the clinical workflow (Soroush et al., 2025).
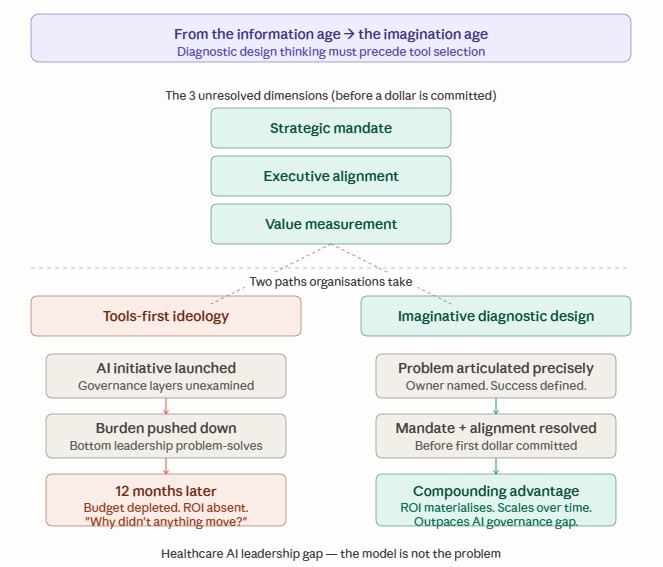
2. Problem Statement
Healthcare organizations deploying AI tools to clinical notes face a documentation layer that was never designed for downstream algorithmic consumption. Three intersecting problems define the scope of the issue.
First, clinical narratives are inherently inconsistent. The same condition is documented differently depending on the author’s training level, specialty, time pressure, and institutional culture. Research using natural language processing to identify stigmatizing language has found that less experienced physicians and those documenting under higher caseload pressure use more judgment-laden language, independent of the patient’s actual clinical status (Sun et al., 2022). When AI models are trained on this corpus, they learn to treat the inconsistency as a clinical signal.
Second, documentation bias is not randomly distributed. It clusters around the same patient populations already affected by structural health inequities. Marginalizing language, including the use of quotation marks to imply disbelief of a patient’s reported symptoms, judgmental descriptors such as “aggressive” or “noncompliant,” and hearsay-style sentence construction, appears disproportionately in the records of Black patients, patients with substance use history, and patients with psychiatric comorbidities (Himmelstein et al., 2022; Pérez et al., 2024). A 2024 retrospective study at an academic emergency department, using large language models to characterize bias at scale, confirmed that negative descriptors are applied unevenly across demographic groups, even when reviewers are blind to the outcome (Suresh et al., 2024).
Third, the downstream consequences are measurable and clinically material. Stigmatizing language in a chart has been shown to influence subsequent providers who read that chart, shaping their attitudes toward the patient and their willingness to order appropriate pain management or follow-up care, an effect sometimes called bias propagation through the medical record (Goddu et al., 2018; Barcelona et al., 2024). When that same biased narrative becomes training data, model input, or retrieval context for a generative AI system, the bias does not remain confined to a single encounter. It is encoded into a reusable artifact that can influence every future prediction, summary, or recommendation the model produces for similarly described patients (Ferryman et al., 2023).
3. Identified Risk
Based on the background research and the problem statement illustration, the risk and impact pathway from documentation bias to organizational and patient harm follows a consistent pattern, which is summarized in the table below.
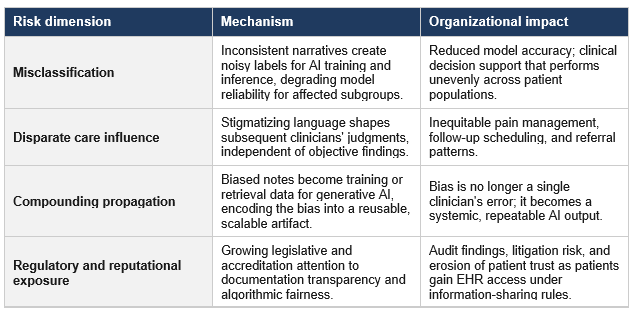
Dr. Kothapalli highlights that inconsistent clinical narratives introduce misclassification errors by generating noisy or inaccurate labels that AI models use during training and inference. This reduces predictive accuracy and can cause clinical decision support systems to perform unevenly across patient populations. Documentation bias also influences subsequent care decisions. Stigmatizing language and subjective descriptions embedded in clinical notes can shape future clinicians’ perceptions, affecting pain management, follow-up scheduling, referral patterns, and treatment decisions independent of objective clinical evidence. These biases become self-reinforcing as each new provider builds on the existing narrative rather than objectively reassessing the patient’s condition.
The organizational implications become even more significant as healthcare organizations increasingly adopt generative AI and clinical decision support systems. Biased clinical documentation is no longer confined to an individual patient encounter; it becomes part of the training corpus for machine learning models, allowing historical inequities to be encoded into scalable AI applications and repeatedly propagated across thousands of future decisions. This compounding effect elevates documentation bias from a documentation quality issue to an enterprise AI governance challenge. At the same time, growing regulatory expectations surrounding algorithmic transparency, fairness, and explainability expose organizations to increased audit scrutiny, legal liability, and reputational risk. As patients gain greater access to their electronic health records and regulators demand greater accountability for AI-enabled healthcare decisions, organizations must implement robust documentation governance, bias detection, and continuous quality improvement strategies to protect both patient trust and the integrity of AI-driven clinical systems.
✦ ✦✦ What Dr. Kothapalli Advocates:
- Proposed AI Solution
The same natural language processing capability that can propagate documentation bias can also be deployed deliberately to detect and mitigate it. A growing body of applied research demonstrates a workable three-layer AI intervention model.
The first layer is detection. NLP classifiers trained specifically to recognize categories of stigmatizing or inconsistent language, including marginalizing language, credibility-questioning phrasing, and judgment-laden descriptors, can be run against clinical notes at scale. The Characterization of Stigmatizing Language in Medical Records project demonstrated that supervised neural classifiers can reliably identify these patterns across large discharge-note corpora, providing a foundation for systematic, ongoing surveillance rather than one-off chart audits (Sushil et al., 2023). The Mount Sinai FAIR Documentation Workgroup extended this approach into a large-scale production pipeline for a large language model capable of characterizing bias across an entire emergency department’s documentation, turning the work into an operational tool (Suresh et al., 2024).
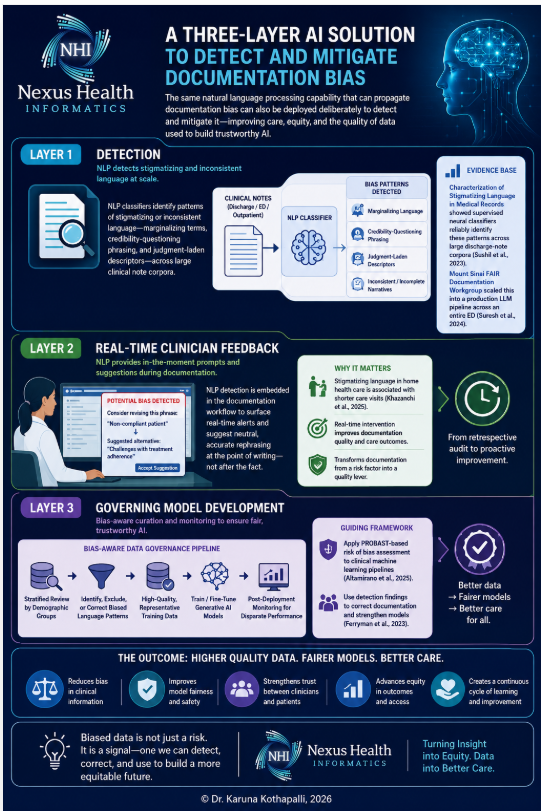
The second layer is real-time clinician feedback. Rather than auditing notes retrospectively, emerging systems such as the ENGAGE protocol propose embedding NLP-based detection of stigmatizing language directly into the documentation workflow, surfacing a prompt or suggested rephrasing to the clinician at the point of writing. Early evidence from home health care settings found that stigmatizing language was associated with measurably shorter care visits, making point-of-documentation intervention a direct lever on care quality and not merely a record-keeping concern (Khazanchi et al., 2025).
The third layer is governing model development. Before any clinical note corpus is used to train or fine-tune a generative AI system, organizations should apply bias-aware data curation: stratified review of training data by patient demographic group, exclusion or correction of identified stigmatizing language patterns, and post-deployment monitoring of model outputs for disparate performance across subgroups, consistent with the PROBAST-based risk of bias assessment frameworks now being applied to clinical machine learning pipelines (Altamirano et al., 2025). Treating biased data as an informative artifact to be corrected, rather than simply discarded or ignored, allows the organization to use detection findings to improve both the documentation culture and the model itself (Ferryman et al., 2023).
2. Data Governance Strategy
A sustainable response to Documentation Bias requires a data governance strategy that operates upstream of any individual AI deployment. The following five components form a practical starting framework for healthcare organizations and AI governance committees.
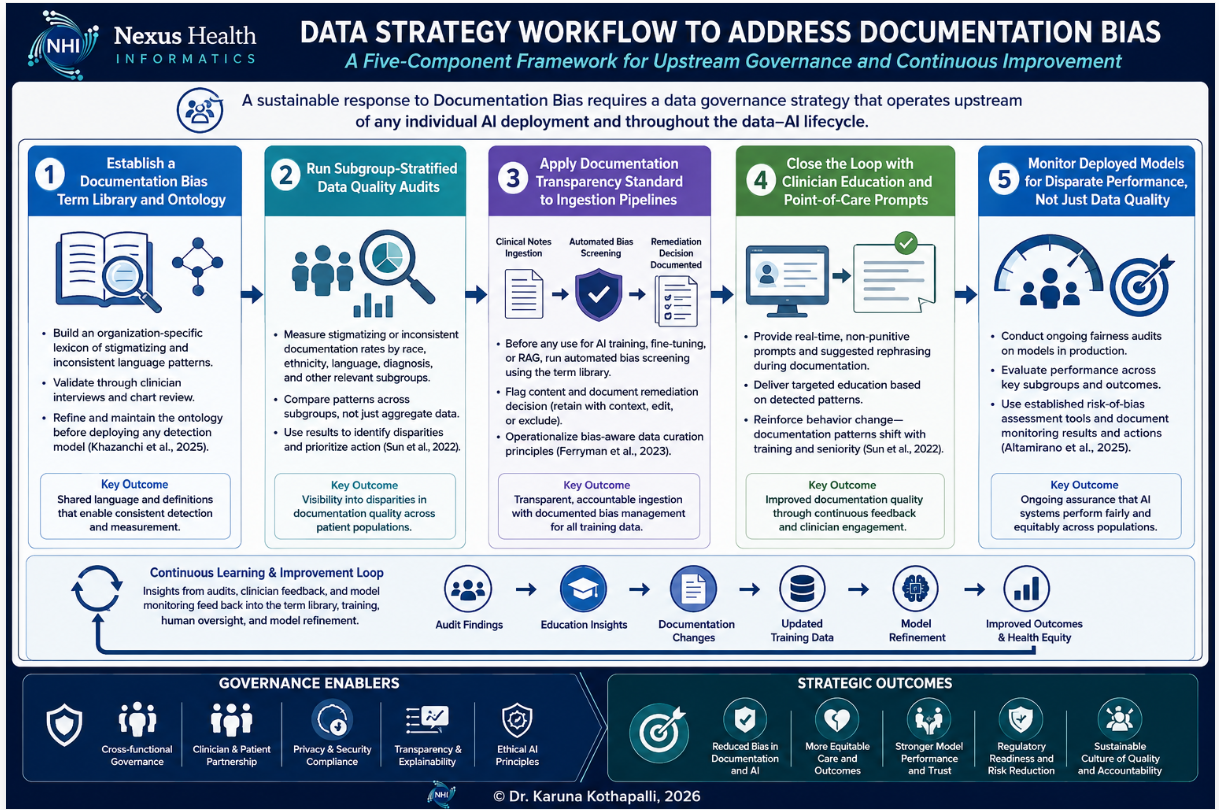
Dr. Kothapalli illustrates in the above infographic that a proactive data governance strategy should address documentation bias before it becomes embedded in artificial intelligence models and clinical decision support systems. Rather than treating bias as a downstream model performance issue, the framework establishes governance at the source of data creation through five interconnected components. It begins by developing a standardized documentation bias ontology to consistently identify stigmatizing and inconsistent language across clinical narratives.
Organizations then conduct subgroup-stratified data quality audits to uncover disparities that may be masked by aggregate metrics. Before clinical notes are used for AI training or retrieval, automated bias screening and documented remediation decisions ensure transparency and accountability throughout the data ingestion process. Detection findings are subsequently translated into targeted clinician education and real-time documentation prompts, creating a continuous feedback mechanism that improves documentation practices at the point of care.
Finally, fairness monitoring extends beyond data quality by evaluating deployed AI models for disparate performance across patient populations, ensuring that improvements in documentation translate into equitable and trustworthy AI outcomes. Collectively, this governance lifecycle transforms documentation bias from an overlooked data quality concern into a measurable, continuously monitored organizational capability that strengthens clinical documentation, enhances AI reliability, supports regulatory compliance, and advances equitable patient care.
✦ ✦✦ Wrap-up – Dr. Kothapalli’s Insights:
Documentation is the first clinical decision made about a patient. When documentation contains bias, every downstream decision, whether human or AI-assisted, inherits that bias. Governance must therefore begin with the clinical narrative, not the algorithm.
- Address documentation bias before data enters AI pipelines, rather than correcting model errors after deployment.
- Every clinical note becomes future training data. Improving documentation today improves AI performance tomorrow.
- Documentation bias is not simply detected; it is governed through a continuous quality improvement cycle that strengthens both clinical documentation and AI performance.
- Bias cannot be eliminated by better algorithms alone. It is reduced through better documentation, stronger governance, and continuous learning across the entire AI lifecycle.
- AI identifies patterns. Clinicians improve documentation. Governance ensures accountability.
If you found this analysis valuable, follow my continuing series on Healthcare AI Ethics and subscribe to the CMS ePriorAuth Interop newsletter.
Check out Series #1 of the Healthcare AI Ethics: https://www.linkedin.com/pulse/healthcare-ai-ethics-weekly-series-1-dr-karuna-kothapalli-4dm4c/
Check out Series #2 of the Healthcare AI Ethics: https://www.linkedin.com/pulse/healthcare-ai-ethics-weekly-series-2-dr-karuna-kothapalli-jykmc/
Check out Series #3 of the Healthcare AI Ethics: https://www.linkedin.com/pulse/healthcare-ai-ethics-weekly-series-3-dr-karuna-kothapalli-revqc/
References:
Altamirano, S., Vreeken, A., & Ghebreab, S. (2025). Machine learning and public health: Identifying and mitigating algorithmic bias through a systematic review. arXiv preprint. https://arxiv.org/pdf/2510.14669
Barcelona, V., Scharp, D., Idnay, B. R., Moen, H., Goffman, D., Cato, K., & Topaz, M. (2024). A qualitative analysis of stigmatizing language in birth admission clinical notes. Nursing Inquiry. https://doi.org/10.1111/nin.12557
Ferryman, K., Mackintosh, M., & Ghassemi, M. (2023). Considering biased data as informative artifacts in AI-assisted health care. New England Journal of Medicine, 389(9), 833–838.
Goddu, A. P., O’Conor, K. J., Lanzkron, S., Saheed, M. O., Saha, S., Peek, M. E., Haywood, C., & Beach, M. C. (2018). Do words matter? Stigmatizing language and the transmission of bias in the medical record. Journal of General Internal Medicine, 33(5), 685–691.
Himmelstein, G., Bates, D., & Zhou, L. (2022). Examination of stigmatizing language in the electronic health record. JAMA Network Open, 5(1), e2144967. https://pmc.ncbi.nlm.nih.gov/articles/PMC8796019/
Khazanchi, R., et al. (2025). Identifying and reducing stigmatizing language in home health care with a natural language processing–based system (ENGAGE): Protocol for a mixed methods study. JMIR Research Protocols. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12511817/
Pérez, T., et al. (2024). Identifying stigmatizing language in clinical documentation: A scoping review of emerging literature. PLOS ONE, 19(6), e0303653. https://journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0303653
Soroush, A., et al. (2025). The use of large language models in clinical documentation: A scoping review. International Journal of Medical Informatics. https://www.sciencedirect.com/science/article/pii/S0020748925003323
Sun, M., Oliwa, T., Peek, M. E., & Tung, E. L. (2022). Negative patient descriptors: Documenting racial bias in the electronic health record. Health Affairs, 41(2), 203–211.
Sushil, M., et al. (2023). Characterization of stigmatizing language in medical records. Proceedings of the 61st Annual Meeting of the Association for Computational Linguistics. https://aclanthology.org/2023.acl-short.28/
Suresh, H., et al. (2024). Identifying and characterizing bias at scale in clinical notes using large language models. medRxiv preprint. https://www.medrxiv.org/content/10.1101/2024.10.24.24316073.full.pdf
Thank you for reading. The leaders who move now will define the standard of care for the next decade. If modernizing your organization’s approach to healthcare innovation is a priority, I’d welcome the opportunity to be part of that journey, architecting the roadmap and structuring the implementation.
Book a convenient time directly in my calendar using my Zoom scheduler here: https://scheduler.zoom.us/dr-karuna-kothapalli
Otherwise, DM me or contact me at karunak@nexushealthinformatics.com