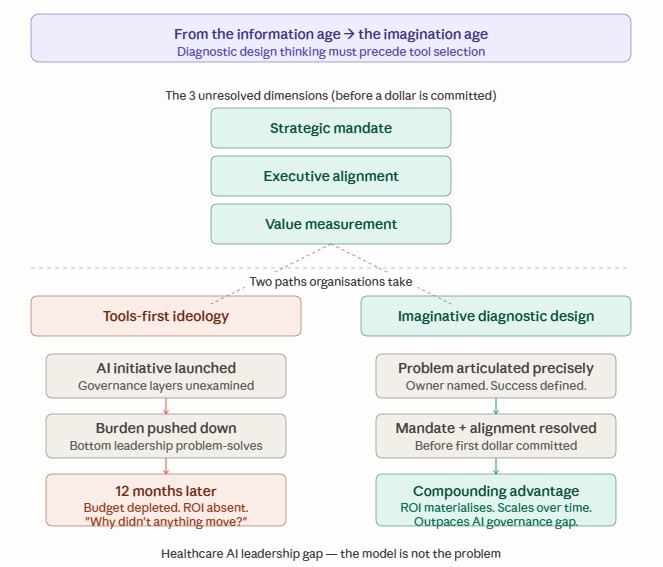
In the weeds, on purpose. This is where trust in clinical AI is actually built or quietly lost.
Yesterday, deep in building the data ingestion for my clinical bias audit pipeline in Claude Science, I hit a decision so small that most people would never notice it was a decision at all. It took thirty seconds to resolve. And it is exactly the kind of moment that determines whether a clinical AI system can be trusted.
Here is what happened. As the pipeline joined clinical notes to their hospital admission records, one note had no match. An orphan. Its admission record simply was not there. This is mundane. Real data is messy, and unmatched records happen constantly.
The traditional default engineering move is to drop it, which I have witnessed for years. You all might have heard these statements: “It does not join cleanly; it complicates the dataset, so you quietly remove it and move on.” The numbers get tidier. The pipeline runs more smoothly. Almost no one would question it, and the status quo would hold.
However, I refused to drop it.
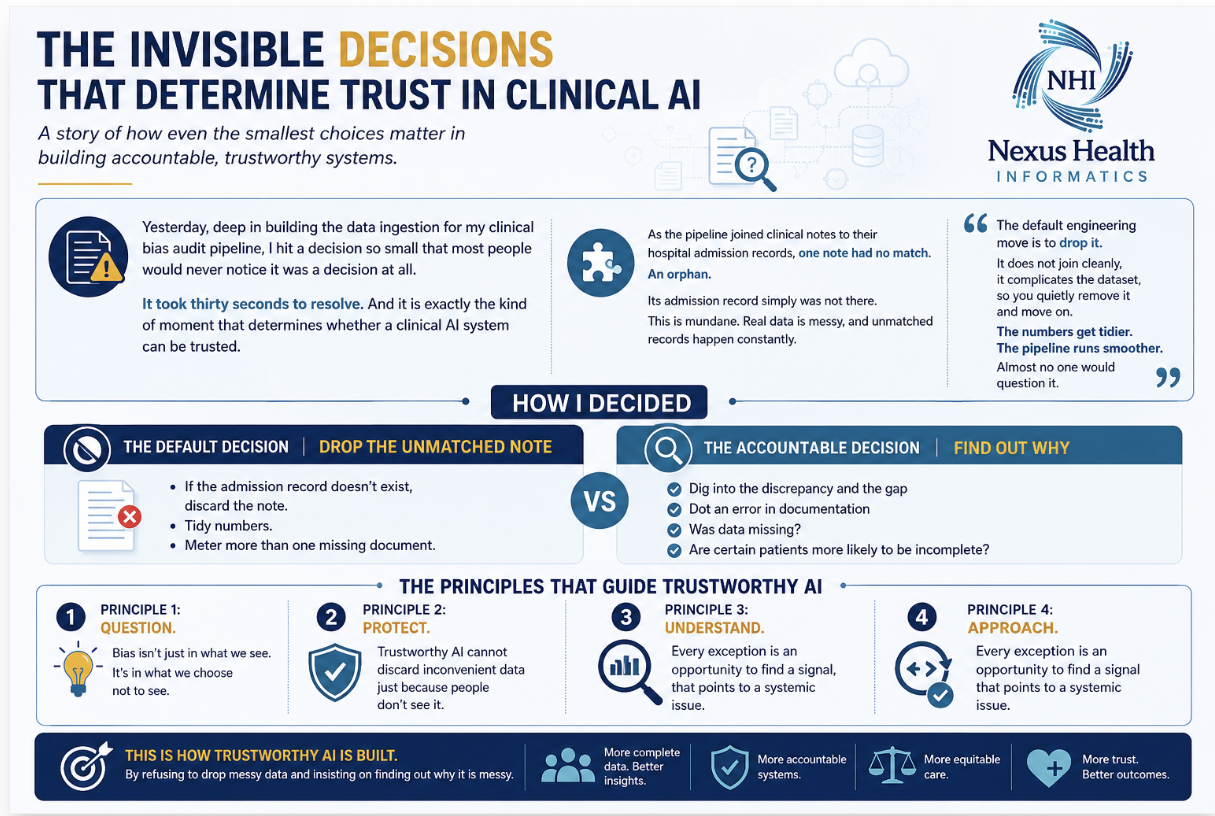
The above infographic paints the picture that, instead, the pipeline keeps that orphaned record, fills its missing fields with explicit nulls, and flags it in the provenance trail so anyone reviewing the audit can see exactly what happened and why. Nothing disappears silently.
Why does this small choice matter so much? Because in a tool whose entire purpose is to measure bias, a silently dropped record is not a cleanup. It is a bias. Every record you quietly remove is a patient you have decided does not count, and you have made that decision invisibly, where no one can see it or challenge it. The patients most likely to have messy, incomplete, orphaned records are often the very patients already underserved by the system. Drop them for tidiness, and your bias audit has itself become biased, in exactly the direction it was built to detect.
This is the quiet signal beneath the loud problem. Everyone talks about algorithmic bias in the model. Far fewer talk about the dozens of invisible decisions upstream, in how the data is cleaned, joined, and filtered, that shape what the model ever sees. A biased model is often just a faithful student of a quietly biased dataset (Suresh & Guttag, 2021). And the bias frequently enters not through some dramatic flaw, but through a hundred thirty-second decisions that no one wrote down.

The lesson coded in the above infographic extends well beyond a single orphaned record. Every transformation in a data pipeline, every join, filter, imputation, exclusion, and normalization represents a governance decision that shapes what the AI system ultimately learns. These decisions are rarely visible to clinicians, executives, or patients, yet they determine whose experiences are represented, whose outcomes are measured, and whose voices become part of the evidence base. Trustworthy AI is therefore not built solely through sophisticated algorithms or fairness metrics, but through transparent, accountable data stewardship from the very first step of the pipeline. When every exception is preserved, documented, and explainable, organizations create an auditable chain of evidence that strengthens scientific integrity, supports equitable care, and enables AI systems to produce insights that healthcare leaders can trust.
The most consequential biases rarely enter an AI system through dramatic failures. They emerge through hundreds of seemingly insignificant engineering decisions that quietly shape the data before a model is ever trained. Responsible AI begins by listening to these whispers, documenting every decision, and ensuring that no patient disappears simply because their data was inconvenient.
That is the discipline I care about, and it is why I build the way I do. Hear the quiet signal before it becomes a roar. Keep what others discard. Flag what others hide. Make every decision visible, so it can be questioned.
Trust in clinical AI is not built into the model. It is built here, in the weeds, in the records we refuse to drop.
This is the first in a recurring series where I share the small, unglamorous decisions from building a clinical bias audit pipeline, and why each one determines whether the result can be trusted. Not the code. The judgment. Follow along, the wins and the honest struggles alike, and I would genuinely value your perspective, especially if you work where clinical data becomes clinical AI.
View my website, nexushealthinformatics.com/hackathon, for daily learning updates.
References:
Suresh, H., & Guttag, J. (2021). A framework for understanding sources of harm throughout the machine learning life cycle. Communications of the ACM, 64(2), 36-46. https://doi.org/10.1145/3465416
#ResponsibleAI #HealthcareAI #ClinicalAI #HealthEquity #AIGovernance #ClinicalDocumentation #BiasInAI #NexusHealthInformatics #WhisperResponsiveLeadership #BuiltWithClaude
Thank you for reading. The standard of care for the next decade is being set right now by the organizations disciplined enough to hear the quiet signals in their data and act before they become liabilities. If building that discipline is a priority, this is exactly the work I do, from roadmap through implementation. I would welcome the conversation.
Book a convenient time directly in my calendar using my Zoom scheduler here: https://scheduler.zoom.us/dr-karuna-kothapalli
Otherwise, DM me or contact me at karunak@nexushealthinformatics.com