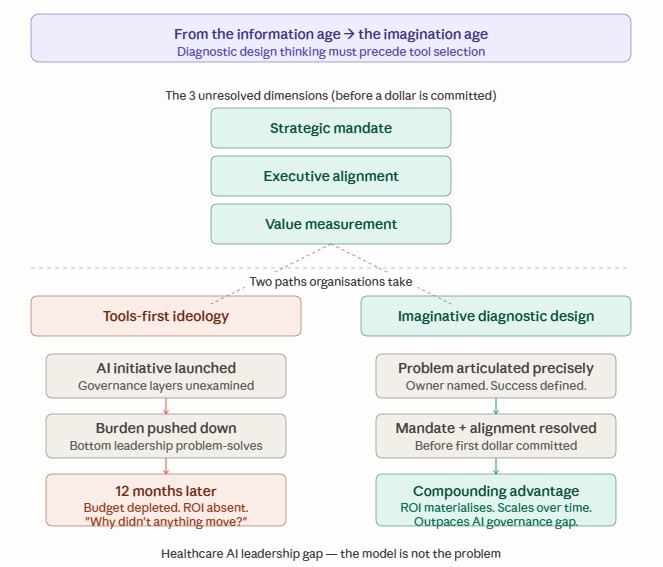
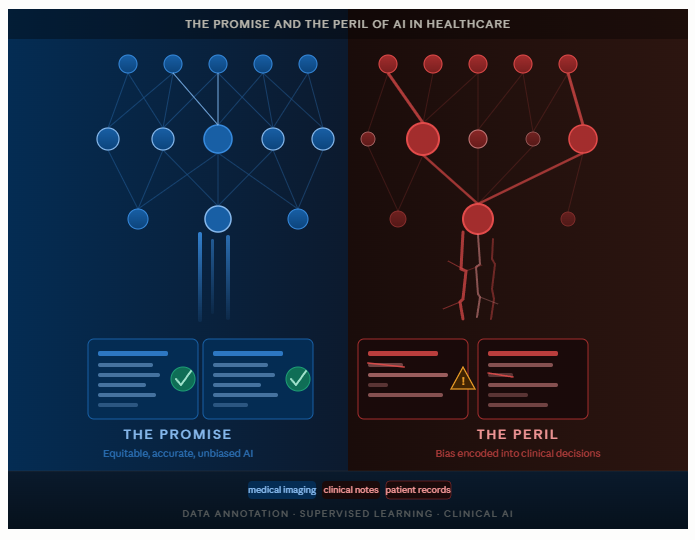
Background: The Promise and the Peril of AI in Healthcare
Artificial intelligence is rapidly transforming healthcare — from diagnostic imaging and clinical decision support to drug discovery and personalized medicine. According to Global Research (2025), for the forecast period 2026–2033, the global AI in healthcare market was valued at approximately USD 36.67 billion and projected to grow to USD 505.59 billion by 2033. Hospitals, insurers, and research institutions are racing to embed machine learning into their workflows, promising faster diagnoses, reduced medical errors, and more equitable care.
Yet beneath this optimism lies a structural vulnerability that too few decision-makers fully appreciate: AI systems are only as unbiased as the data and human judgments used to train them. In healthcare, where data annotation — the labeling of medical images, clinical notes, and patient records that underpins every supervised learning model can quietly encode cultural, racial, gender, and socioeconomic prejudices directly into clinical AI.
This article examines one of the most underappreciated yet consequential sources of AI failure in medicine: human and labeling bias—the systematic distortions that emerge when annotators bring their own worldviews to the task of labeling training data.
Annotators Are Not Neutral: The Human in the Loop
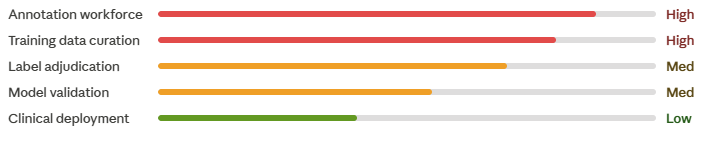
Supervised machine learning, the dominant paradigm in clinical AI, requires vast quantities of labeled data. A dermatology AI must learn from thousands of dermatologist-labeled skin lesion images. A sepsis prediction model must train on electronic health records annotated by clinicians. A radiology algorithm must study chest X-rays marked by radiologists. In each case, the model learns to replicate human judgment — and if that judgment is systematically biased, the model will be too.
Labeling bias arises when annotators apply subjective judgments that reflect cultural norms, personal experiences, implicit attitudes, or institutional conventions rather than objective clinical truth. Unlike random annotation error, labeling bias is systematic and directional, consistently skewing outputs against identifiable patient groups.
Research has documented several overlapping mechanisms through which this occurs:
• Pain Underestimation Bias: Studies show that clinicians systematically underestimate pain in Black patients relative to white patients with identical presentations. A 2016 study published in PNAS found that a substantial portion of medical students and residents held false beliefs about biological differences between Black and white patients, such as the myth that Black people have thicker skin leading to undertreated pain (Hoffman et al., 2016). When such practitioners annotate training data, these biases transfer into AI pain assessment tools.
• Gender Bias: Women presenting with acute myocardial infarction are more likely to be misdiagnosed or have their symptoms labeled as anxiety or non-cardiac in origin (Lichtman et al., 2018). AI models trained on historically annotated cardiology records learn to treat atypical (female-typical) MI presentations as lower acuity, propagating diagnostic delays in automated triage systems.
• Socioeconomic and Language Bias: Patients from lower socioeconomic backgrounds or with limited English proficiency may receive less thorough clinical documentation, resulting in data sparsity bias where the AI treats the absence of documented information as the absence of clinical need, effectively penalizing already underserved groups.
Crucially, these biases often become invisible at deployment. Because AI models perform well on benchmark datasets themselves labeled by the same biased processes, developers may not detect the problem until the model harms patients in real clinical environments.
The Stakes: Patient Safety, Equity, and Trust
The consequences of unchecked labeling bias in healthcare AI span clinical, ethical, legal, and systemic dimensions:
1. Clinical Harm and Patient Safety
When biased labels are used to train a clinical AI, the resulting model may systematically underperform for certain patient populations. An AI dermatology tool trained predominantly on lighter skin tones, which is a known issue (Daneshjou et al., 2022), exhibits significantly lower diagnostic accuracy for melanoma in patients with darker skin. In a clinical setting where AI output influences biopsy decisions, this translates directly into delayed cancer diagnoses and preventable deaths among patients of color.
3. Erosion of Trust in AI and Digital Health
Trust is the currency of healthcare. When patients, particularly those from historically marginalized communities, learn that AI tools may be systematically less accurate or fair for them, the result is justified skepticism toward digital health broadly (Nazer et al., 2023). This erosion of trust threatens the adoption of beneficial AI technologies and may drive patients away from care altogether.
4. Misallocation of Healthcare Resources
At a systems level, biased AI can misdirect diagnostic resources, clinical interventions, and public health spending away from populations with the greatest need — worsening population health outcomes while increasing overall costs through missed early diagnoses and undertreated chronic disease.
What Must Be Done: A Framework for Equitable AI Annotation
Addressing labeling bias requires coordinated action across the AI development lifecycle, from data collection through deployment and monitoring. Some of the following evidence-based recommendations reflect emerging best practices in algorithmic fairness and responsible AI in medicine.
- Diverse Annotator Panels: According to Gebru et. al. (2021), recruit annotators that reflect the demographic and cultural diversity of the patient populations the AI will serve. Track and report annotator demographics as part of dataset documentation (“datasheets for datasets”).
- Structured Annotation Protocols: Develop annotation guidelines that explicitly define clinical criteria, reduce reliance on subjective interpretation, and include training modules on implicit bias and cultural competency for all annotators.
- Measure and Report Inter-Annotator Agreement: Publish inter-annotator reliability metrics (Cohen’s kappa, Fleiss’ kappa) stratified by patient demographic subgroups. Low agreement within specific groups is a signal of labeling bias that warrants investigation.
- Bias-Aware Ground Truth Construction: Move beyond simple majority-vote labeling. Use techniques such as Dawid-Skene modeling, crowd-truth, or Bayesian annotation models that weight annotator reliability and flag systematic disagreement patterns.
✦ For Healthcare Organizations and Clinical Leaders
• Demand Bias Documentation: Require vendors to provide model cards and bias audit reports as conditions of procurement. Do not deploy AI tools that cannot demonstrate equitable performance across patient subgroups.
• Invest in Representative Data Infrastructure: Support initiatives to collect and curate training datasets that represent underrepresented populations, including community health center data, safety net hospital records, and international datasets for global-use models.
• Establish AI Ethics Committees: Create governance structures including clinical ethicists, patient advocates, and community representatives with authority to review, pause, or reject AI deployments that exhibit discriminatory performance.
• Train Clinical Staff on AI Limitations: Ensure that clinicians using AI decision support understand that model outputs are probabilistic, may be less reliable for underrepresented populations, and should never override clinical judgment and patient context.
✦ For Policymakers and Regulators
• Mandate Pre-Market Bias Auditing: Regulatory bodies (FDA, EMA, MHRA) should require prospective bias audits stratified by race, sex, and socioeconomic status as part of the approval pathway for high-risk clinical AI systems.
• Fund Equity-Centered AI Research: Increase NIH, AHRQ, and NSF funding for research into algorithmic fairness, inclusive dataset curation, and bias mitigation techniques specifically applied to clinical AI.
• Protect Annotation Workers: Recognize medical data annotators as skilled healthcare workers. Establish professional standards, fair compensation, and mental health support for annotators, particularly those reviewing sensitive clinical content.
✦ For Patients and Communities
• Advocate for Algorithmic Transparency: Patients have the right to know when AI informs their care and to request information about how AI tools were validated across demographic groups.
• Participate in Data Donation Programs: Community engagement in medical data collection and annotation — with appropriate consent, privacy protections, and community benefit agreements — helps build the representative datasets that equitable AI requires.
✦ ✦✦ What Dr. Kothapalli Advocates:
Annotator diversity by race, gender, specialty, geography, and patient population served should be a procurement standard, not a nice-to-have. Platforms that source clinical labels must audit and report annotator demographics, as trials report participant demographics.
Regulatory approval and clinical deployment should require performance stratified by race, gender, age, and socioeconomic status—not as supplementary analyses, but as primary endpoints. Every clinical AI system should architect a structured disclosure: who labeled the data, what populations were represented, how inter-rater disagreements were resolved, and where performance gaps exist. Transparency is a precondition for accountability.
Conclusion
AI in healthcare holds genuine transformative potential — but only if we are willing to confront the human biases embedded in the data that trains it. Labeling bias is not a technical edge case; it is a fundamental structural challenge that sits at the intersection of data science, medical culture, and social equity. When annotators encode their prejudices into training data, they do not simply make a model less accurate — they create a system that may actively harm the most vulnerable patients.
References:
Grand View Research. (2025). AI in Healthcare Market Size, Share & Trends Analysis Report. Grand View Research, Inc. https://www.grandviewresearch.com/industry-analysis/artificial-intelligence-ai-healthcare-market
Hoffman, K. M., Trawalter, S., Axt, J. R., & Oliver, M. N. (2016). Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between Blacks and Whites. Proceedings of the National Academy of Sciences, 113(16), 4296–4301. https://doi.org/10.1073/pnas.1516047113
Litchman, J., Leifheit, E. C., Safdar, B., Bao, H., Krumholz, M. H., Lorenze, P. N., Daneshvar, M., Spertus, A. J., & D’Onofrio, G. (2018). Sex Differences in the Presentation and Perception of Symptoms Among Young Patients With Myocardial Infarction. Circulation, 137(8), 781–790. https://doi.org/10.1161/CIRCULATIONAHA.117.031650
Daneshjou, R., Vodrhahalli, K., Novoa, R., Jenkins, M., Liang, W., Rotemberg, V., Ko, J., Swetter, M. S., Bailey, E., Gevaert, O., Mukherjee, P., Phung, M., Yekrang, K., Fong, B., Sahasrabudhe, R., Allerup, A. C. J., Okata-Karigani, U., Zou, J., & Chiou, S. J. (2022). Disparities in dermatology AI performance on a diverse, curated clinical image set. Science Advances, 8(32). https://doi.org/10.1126/sciadv.abq6147
Nazer, H. L., Zatarah, R., Waldrip, Shai., Ke, C. K. J., Moukheiber, M., Khanna, K. A., Hicklen, S. Rachel., Moukheiber, L., Moukheiber, D., Ma, & Mathur, P. (2023). Bias in artificial intelligence algorithms and recommendations for mitigation. PLOS Digital Health, 2(6), e0000278. https://doi.org/10.1371/journal.pdig.0000278
Gebru, T., Morgenstern, J., Vaughan, W. J., Wallach, H., Daume III, H., & Crawford, K. (2021). Datasheets for Datasets. Communications of the ACM, 64(12), 86–92. https://doi.org/10.1145/3458723
#AIBiasInHealthcare #HealthEquity #ResponsibleAI #MedicalAI #AlgorithmicFairness #AI Ethics
Thank you for reading. Biased AI doesn’t announce itself — it surfaces in missed diagnoses, skewed risk scores, and care gaps that fall hardest on those already underserved. The organizations that lead on data modernization with built-in equity frameworks will set the standard for a decade of responsible healthcare AI.
If your organization is ready to move from awareness to action — designing AI systems that are transparent, auditable, and equitable — I’d love to help architect that roadmap and guide the implementation.
Book a convenient time directly in my calendar using my Zoom scheduler here: https://scheduler.zoom.us/dr-karuna-kothapalli
Otherwise, DM me or contact me at karunak@nexushealthinformatics.com