
Every clinician knows the drill. A patient needs a procedure. You pick up the phone, navigate a payer’s IVR, wait on hold, fax forms, refresh a portal, and hours later, maybe you have an answer.
Prior authorization has become one of healthcare’s most expensive and demoralizing rituals.
That ritual is now on borrowed time.
1. The CMS Mandate: What Changed and Why It Matters
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) fundamentally rewrites how prior authorization must work across the U.S. healthcare system. This is not a pilot program or voluntary initiative — it is a regulatory mandate with teeth.
Personal Insight
What strikes me most about CMS-0057-F is not the technical requirements themselves, but the deliberate sequencing behind them. CMS did not simply hand down a deadline and walk away. The agency built an enforcement architecture — decision timelines already in effect for 2026, API mandates landing in 2027, and public metrics reporting layered on top — that creates compounding accountability at every level of the ecosystem.
For health systems and technology leaders still treating this as a compliance checkbox, framing is a costly miscalculation. The organizations moving now are not just avoiding penalties; they are building the interoperability infrastructure that will define competitive positioning in value-based care for the next decade.
The mandate is the floor, not the ceiling.
Let us look at the core requirements and the impacted sub-entities.
Core Requirements
- Decision timelines: Payers must respond within 72 hours for urgent requests and 7 calendar days for standard requests — already in effect for 2026.
- API infrastructure: All impacted payers must implement and maintain FHIR-based Prior Authorization APIs by January 1, 2027.
- Public reporting: Payers are required to publish prior authorization metrics, bringing transparency to a historically opaque process.
- Scope: Applies to Medicare Advantage, Medicaid managed care plans, CHIP, and Qualified Health Plans on federal exchanges.
Who is impacted
The rule touches every layer of the healthcare ecosystem:
- Health plans/payers — must build and expose FHIR APIs.
- EHR vendors — must integrate PA workflows into clinical systems.
- Providers/health systems — must adopt electronic workflows by replacing fax and phone.
- Networks & clearinghouses — must facilitate end-to-end data exchange.

2. The Interoperability & Prior Authorization Framework
Electronic prior authorization does not function in isolation.
It is the centerpiece of a broader interoperability architecture built on the HL7 FHIR (Fast Healthcare Interoperability Resources) standard — a modern, API-first approach to healthcare data exchange.
At its core, FHIR replaces the fragmented, document-heavy workflows that have long defined healthcare administration — faxed forms, proprietary payer portals, phone-based status checks — with structured, machine-readable data exchanged through standardized APIs.
Think of it as giving every participant in the prior authorization chain a common language: providers, payers, EHR systems, and patient applications can all send and receive information in a format that any compliant system can immediately understand and act on.
This shift is not merely technical. When clinical data flows cleanly between systems at the moment it is needed, authorization decisions accelerate, documentation burden drops, and the administrative overhead that consumes thousands of clinician hours each week begins to shrink in a measurable, auditable way.
Personal Insight
When I mapped the four mandated APIs alongside the Da Vinci implementation guides, what became immediately clear is that CMS did not design four independent data pipes — it designed a closed-loop intelligence system.
The Prior Authorization API handles the transaction, but it is the Coverage Requirements Discovery and Documentation Templates and Rules components of Da Vinci that make the transaction nearly invisible to the clinician.
The Provider Access and Payer-to-Payer APIs then ensure that the data driving those decisions travels with the patient across care settings and plan changes, eliminating the information resets that currently force providers to re-document what should already be known.
What I find most significant from an architectural standpoint is that the Da Vinci initiative essentially sits between the mandate and the implementation — translating regulatory intent into working FHIR profiles that EHR vendors and payers can actually build.
Organizations that engage with Da Vinci’s CRD, DTR, and PAS guides now, rather than waiting for their EHR vendor to surface them, will have a meaningful head start in shaping workflows that work for their clinical reality rather than retrofitting a vendor default.
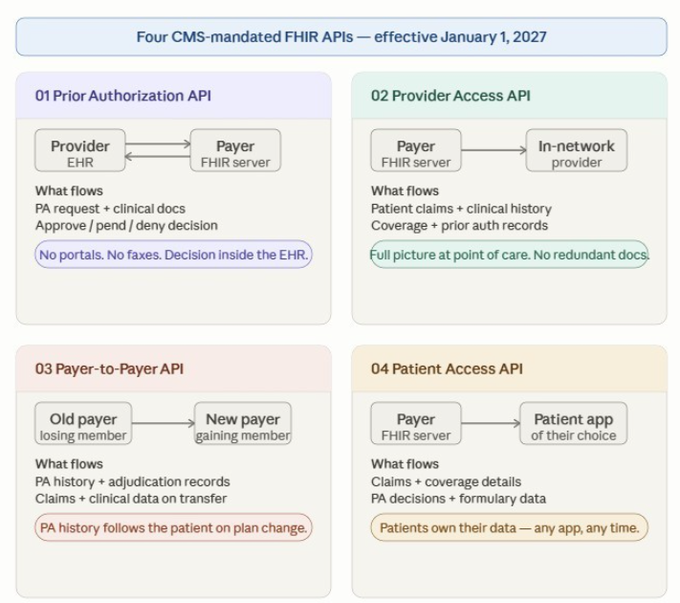
The Four-API Ecosystem
CMS has mandated four interconnected APIs that together create a continuous, end-to-end data layer:
- Prior Authorization API — Providers submit PA requests and receive decisions directly from within their EHR. No portals. No faxes.
- Provider Access API — In-network providers access patient claims and clinical data at the point of care, reducing redundant documentation.
- Payer-to-Payer API — When a patient changes insurers, their prior authorization history transfers automatically between health plans.
- Patient Access API — Patients can download their own claims, coverage details, and PA decision history via apps of their choice.
The Da Vinci Initiative: Industry-Led Standards
The technical implementation relies heavily on HL7’s Da Vinci Project — a collaboration between payers, providers, and EHR vendors to develop FHIR implementation guides (IGs) that translate regulatory requirements into working software:
- Coverage Requirements Discovery (CRD) — Real-time, in-workflow alerts on whether a PA is required for a given service.
- Documentation Templates & Rules (DTR) — Auto-populates PA forms using structured clinical data already in the EHR.
- Prior Authorization Support (PAS) — Routes the completed PA request to the payer and returns a decision in real time.
- Clinical Data Exchange (CDex) — Attaches supporting clinical documentation (C-CDA, PDFs) when the payer requests additional information.
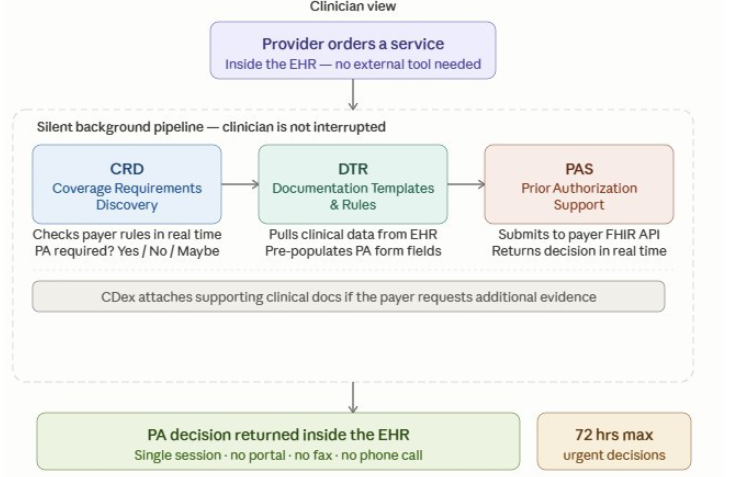
Source: Dr. Karuna Kothapalli, May 2026. The clinician's view is the only visible action; the dashed container shows three Da Vinci components: Coverage Requirements Discovery (CRD), Documentation Templates & Rules (DTR), and Prior Authorization Support (PAS), with Clinical Data Exchange (CDex) operating within the EHR.
Wrap Up
That covers the first two pillars of this series — the regulatory foundation driving the urgency and the interoperability architecture that makes electronic prior authorization technically possible at scale.
What I hope comes through is that these two elements are inseparable: the mandate without the framework is just a deadline, and the framework without the mandate would remain a well-intentioned industry experiment.
Together, they represent the most significant structural shift in healthcare administrative workflow in a generation.
In the next installment, we will go deeper into the API build itself — what technology teams actually need to implement, the Da Vinci implementation guides that translate regulation into working code, and the real-world integration challenges that the 30 early adopter organizations are already working through.
Follow along if you are building, planning, or advising on healthcare interoperability — the runway to 2027 is shorter than it looks. For teams managing EHR integrations and payer contracts, the clock is already running.
Series #1 of the Interoperability & Prior Authorization
Next up: The API Build and Integration Playbook.
The rulebook is written. Now comes the hard part.
Stay tuned for Part 2.
References
- CMS. (2026). 2024 CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F). CMS.GOV. Retrieved May 15, 2026, from https://www.cms.gov/priorities/burden-reduction/overview/interoperability/policies-regulations/cms-interoperability-prior-authorization-final-rule-cms-0057-f
- CMS. (2026). CMS Announces Early Adopters to Advance Solutions for Electronic Prior Authorization, Accelerating Momentum Ahead of 2027 Requirements. CMS.GOV. Retrieved May 15, 2026, from https://www.cms.gov/newsroom/press-releases/cms-announces-early-adopters-advance-solutions-electronic-prior-authorization-accelerating-momentum
- Myers and Stauffer. (2026). Prior Authorization Provisions Implementation Timelines: Update. Retrieved May 15, 2026, from
Prior Authorization Provisions Implementation Timelines: Update
Follow the series:
#PriorAuthorization #HealthIT #FHIR #Interoperability #CMS #HealthcareTechnology #DigitalHealth














